![EOScu Logo - Dark - Outlined [07182023]-01](https://blog.eoscu.com/hubfs/Eoscu_June2024/Images/EOScu%20Logo%20-%20Dark%20-%20Outlined%20%5B07182023%5D-01.svg)


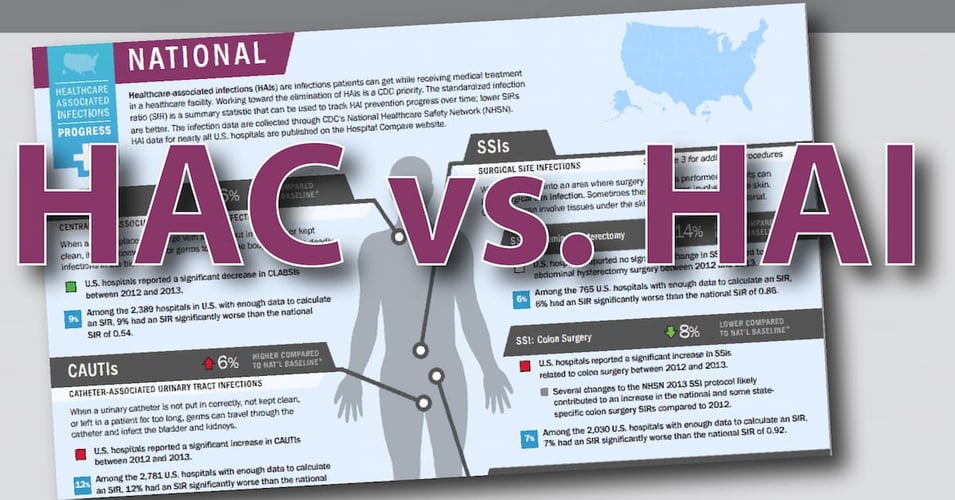
In an effort to reduce patient harm, Medicare continues to penalize hospitals with the highest...
Modifiable Risk Factors: The Courage to Change the Things We Can

The Serenity Prayer is a well-known piece of advice about how to approach life's challenges. In it, the speaker asks for serenity to accept the things that cannot be changed, courage to change the things that can, and wisdom to know the difference. When it comes to infection control, the same sentiment could apply to risk factors. There are some risks that cannot be changed, health challenges that we just have to accept and work around. But there are those we can change, and these are modifiable risk factors. The wisdom to know the difference? We'll try to tackle that topic in today's post.
There are certain risk factors that make some patients more vulnerable to acquiring a healthcare-associated infection. First, let's list all the risks that healthcare professionals in infection control and prevention (IP) cannot impact.
Non-Modifiable Risk Factors
- Patient Age: Newborns and the elderly are at greater risk due to their weaker immune systems.
- Co-morbid conditions or underlying disease: IP can't change the patient's health status or severity while they are receiving treatment.
- Immunosuppressed status: Neither primary nor secondary immunodeficiency can be affected by IP.
- Treatment: IP cannot alter necessary invasive procedures, the need for indwelling devices, or an extended stay in a hospital due to the underlying health condition.
- Post-discharge behavior: While IP can provide extensive patient education, their behavior post-discharge is out of our reach.
After we take a brief moment to take a deep breath and accept that there are things we cannot change, let's dive into some of those things that we can change through interventions that disrupt the three elements needed for an HAI: A source, a host, and a means of transmission.
Modifiable Risk Factors
-
Eliminating sources of pathogens: We can reduce risk by working to eliminate pathogen reservoirs, from surfaces to devices to HCW hands. Environmental services in partnership with IP staff, nurses, and other HCWs ensure that high-touch surfaces are clean. Biocidal materials can reduce biological contamination by continuously killing bacteria.
-
Protecting the potential host: By use of personal protective equipment, isolation, and hand hygiene, we can protect vulnerable patients from pathogens. We can also mitigate some risks brought on by their treatment, such as reducing catheter days and monitoring antibiotic use. Biocidal materials can keep the patient area in the benign zone by continuously killing bacteria.
-
Stopping means of transmission: Technology can provide risk reduction in these areas. Air scrubbers can remove airborne pathogens, while negative air flow reduces the circulation of contaminated air around the patient. Single-use products or patient-dedicated equipment can also reduce the risk of transmission.
Where does courage come in to the equation? It takes courage to stand up for infection control and prevention, in any context. Even in the most successful and well-funded facilities, medical professionals are busy and single-minded, two attributes that can make discussions of infection control protocols and regulations difficult. It takes courage to point out where your facility could do better, courage to ask for funds to cover necessary upgrades to equipment, courage to look your colleagues in the eye and tell them they need to wash their hands. It also takes courage to learn about a new intervention and propose it for your facility, especially when it requires a financial investment.
And now, the wisdom. Where we need wisdom is to see when new interventions and practices make a risk factor actually something we can change, something that we can do to increase better patient outcomes. Where in the past infection itself was seen as a non-modifiable risk of medical treatment, we now know we can reduce the risks. It took generations of physicians to accept this fact, but in time, the shift took place. Perhaps the next shift will be in areas where significant progress has already been made, but where a few courageous individuals say "we can do even better." The result just might be an answered prayer for so many vulnerable patients.
![[infographic] Modes of Transmission Download and share!](https://no-cache.hubspot.com/cta/default/216314/interactive-178287789067.png)
Editor's Note: This post was originally published in August 2019 and has been updated for freshness, accuracy and comprehensiveness.